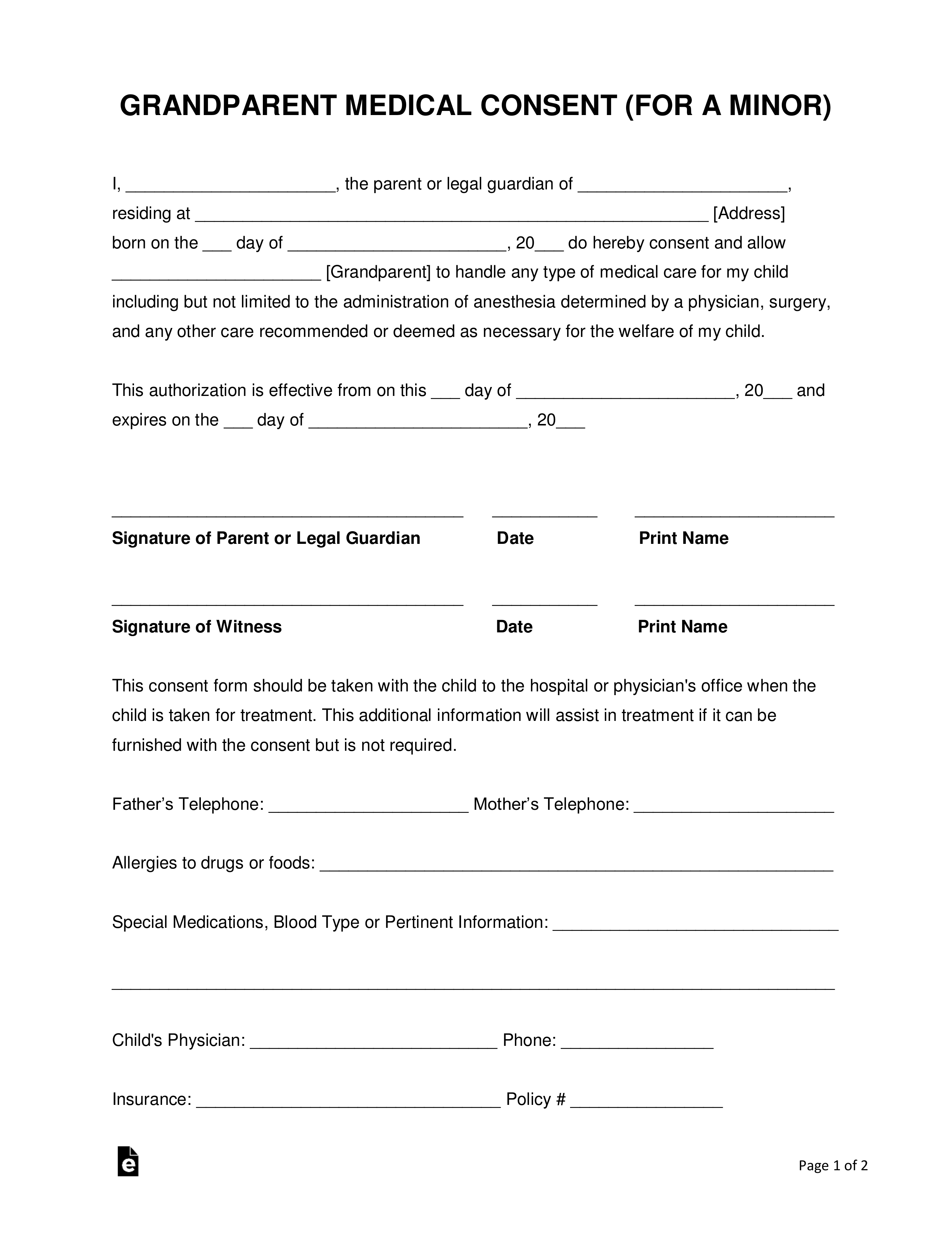
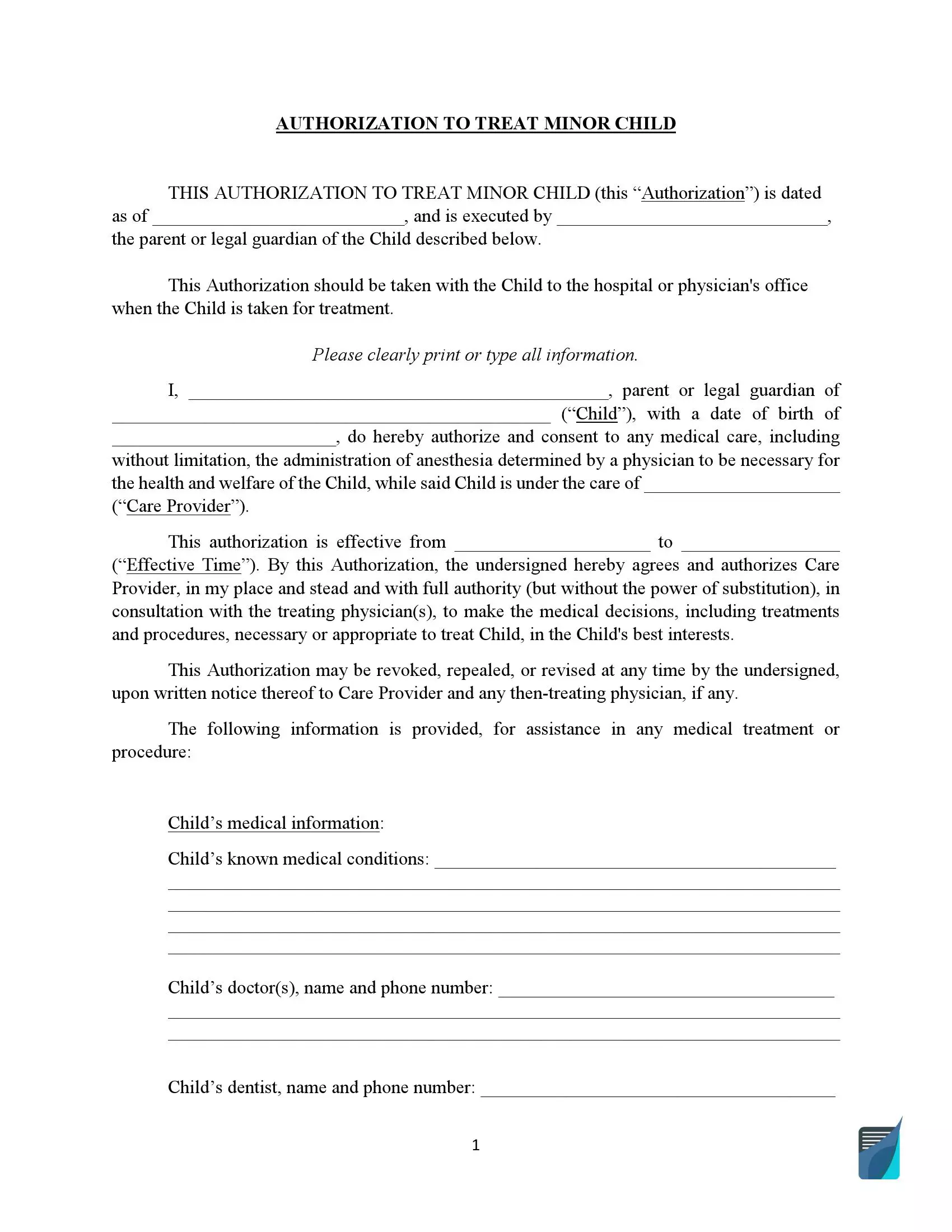
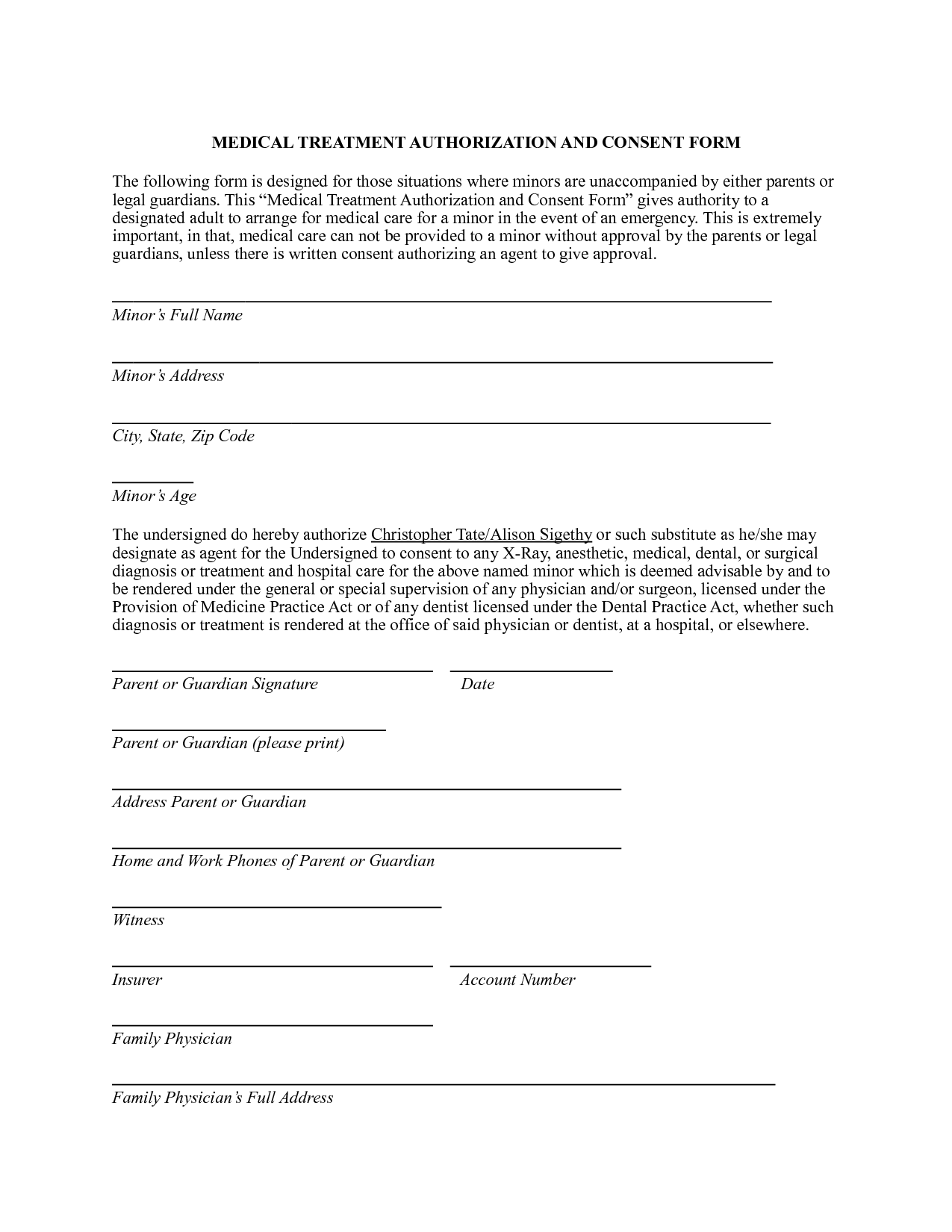
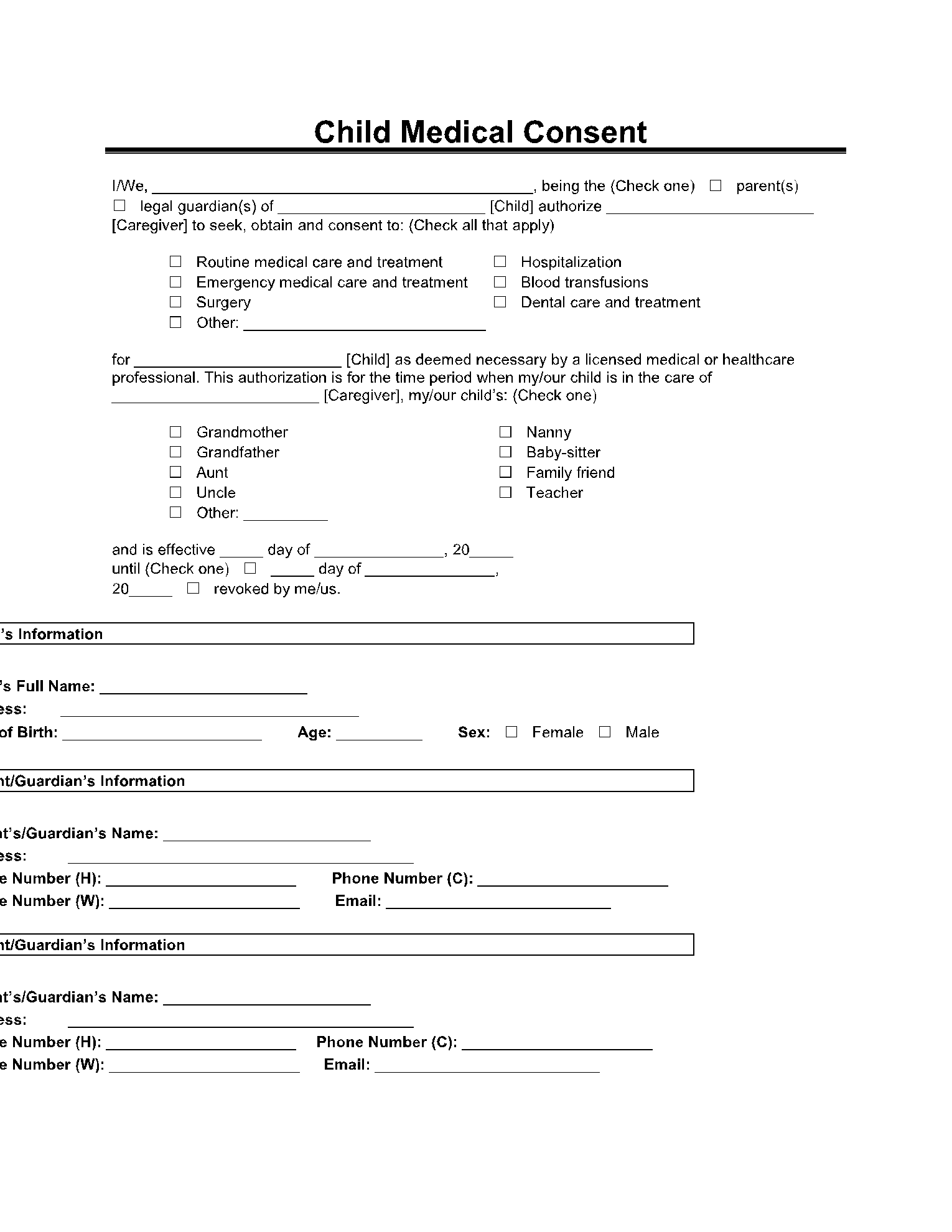
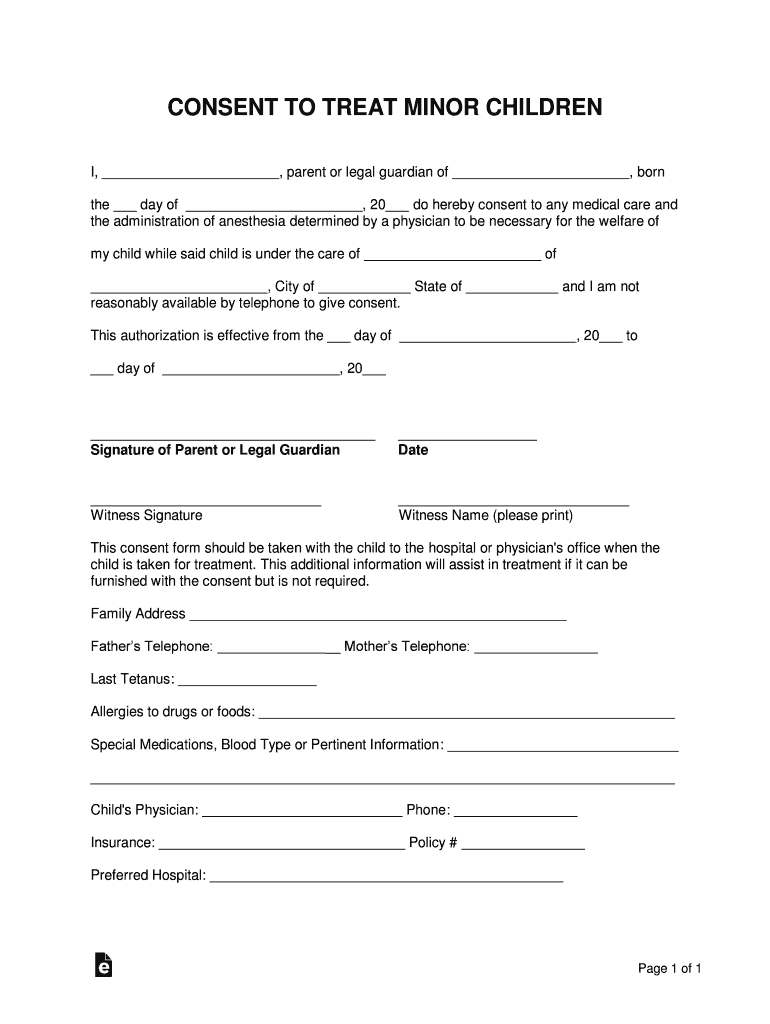
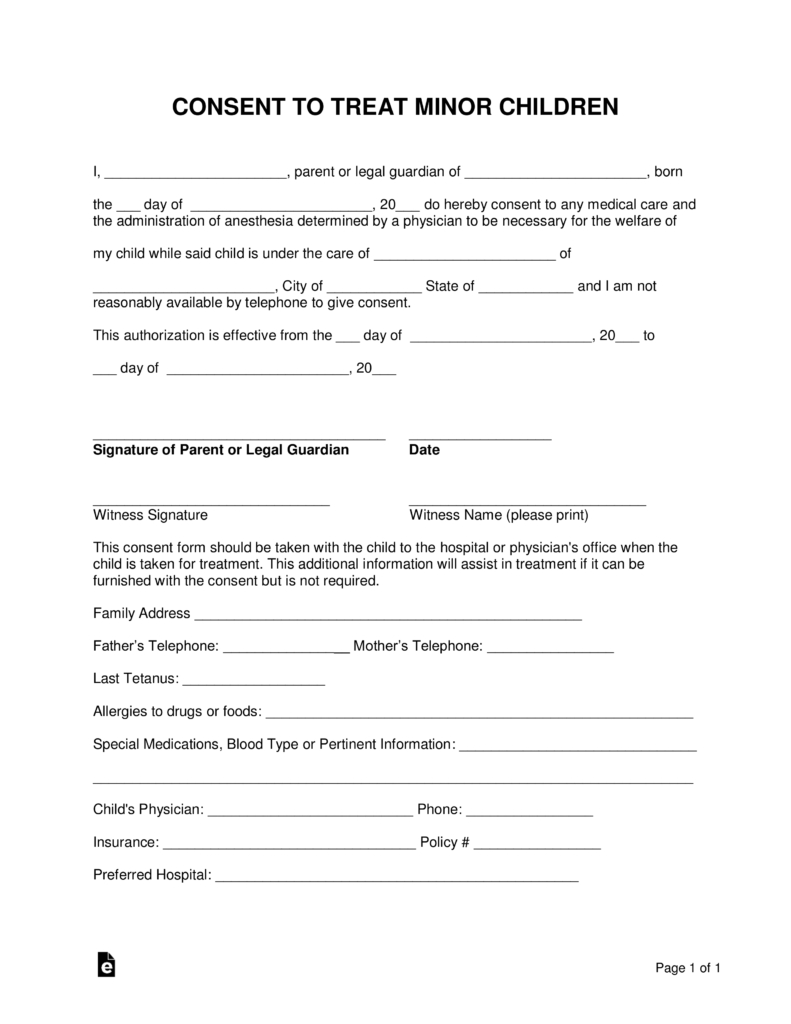
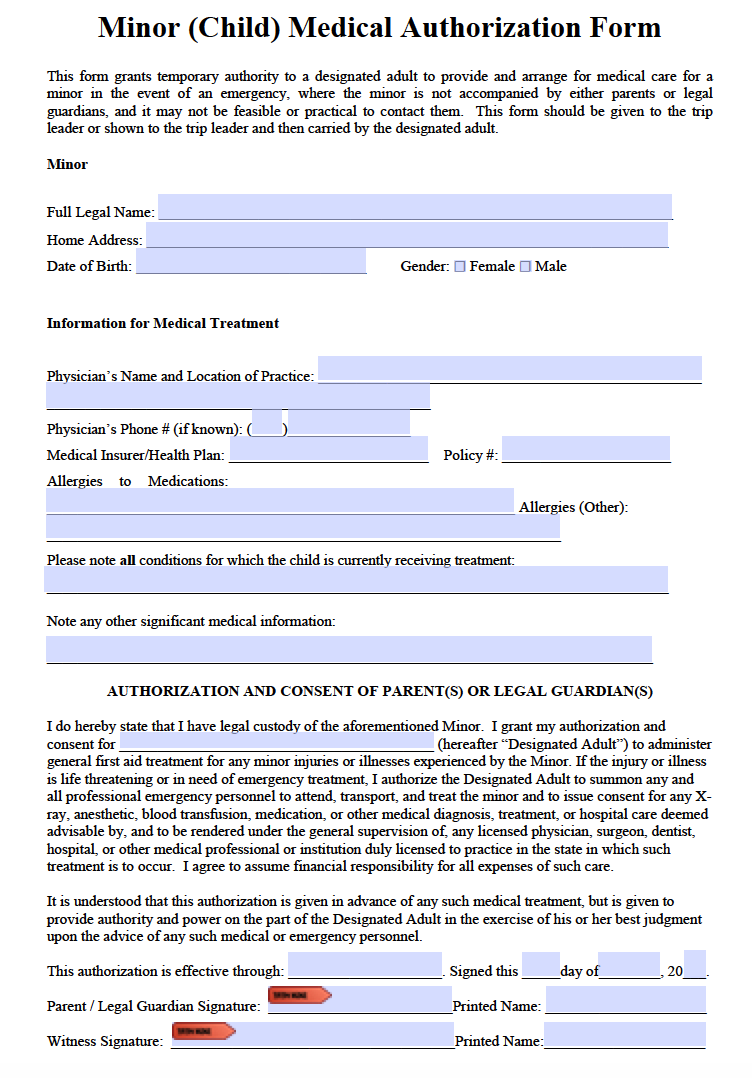
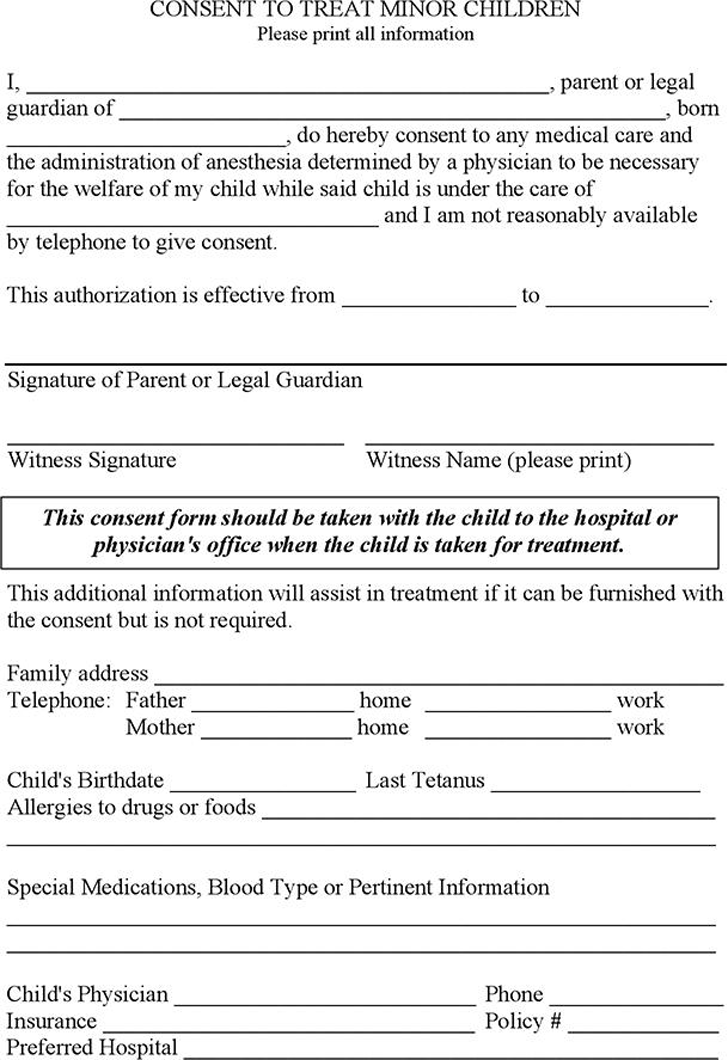
Consent Form For Treatment Of A Minor Without Parent - I authorize the following individual, who is a person over 18. I have the legal right to consent for medical treatment for this child (patient). Check here if you wish to give consent for the minor to receive medical care without an accompanying adult. _____________________________ (name of caregiver) the right to give consent to authorize medical care for the above named minor child. Parent/legal guardian fills out and signs this consent form authorizing up health system medical group clinics to provide treatment to.
_____________________________ (name of caregiver) the right to give consent to authorize medical care for the above named minor child. Check here if you wish to give consent for the minor to receive medical care without an accompanying adult. I authorize the following individual, who is a person over 18. Parent/legal guardian fills out and signs this consent form authorizing up health system medical group clinics to provide treatment to. I have the legal right to consent for medical treatment for this child (patient).
I have the legal right to consent for medical treatment for this child (patient). I authorize the following individual, who is a person over 18. Parent/legal guardian fills out and signs this consent form authorizing up health system medical group clinics to provide treatment to. Check here if you wish to give consent for the minor to receive medical care without an accompanying adult. _____________________________ (name of caregiver) the right to give consent to authorize medical care for the above named minor child.
Medical Treatment Printable Medical Consent Form For Minor
Check here if you wish to give consent for the minor to receive medical care without an accompanying adult. I have the legal right to consent for medical treatment for this child (patient). I authorize the following individual, who is a person over 18. _____________________________ (name of caregiver) the right to give consent to authorize medical care for the above.
Child Medical Consent Form ⇒ Treatment Permission for Minors
Check here if you wish to give consent for the minor to receive medical care without an accompanying adult. I have the legal right to consent for medical treatment for this child (patient). Parent/legal guardian fills out and signs this consent form authorizing up health system medical group clinics to provide treatment to. I authorize the following individual, who is.
Parent Consent Form For Medical Treatment Free Printable Documents
_____________________________ (name of caregiver) the right to give consent to authorize medical care for the above named minor child. Parent/legal guardian fills out and signs this consent form authorizing up health system medical group clinics to provide treatment to. Check here if you wish to give consent for the minor to receive medical care without an accompanying adult. I authorize.
Printable Medical Consent Form For Minor Traveling Without Parents
_____________________________ (name of caregiver) the right to give consent to authorize medical care for the above named minor child. I authorize the following individual, who is a person over 18. Parent/legal guardian fills out and signs this consent form authorizing up health system medical group clinics to provide treatment to. I have the legal right to consent for medical treatment.
Printable Medical Consent Form for Minor While Parents Are Away
Check here if you wish to give consent for the minor to receive medical care without an accompanying adult. _____________________________ (name of caregiver) the right to give consent to authorize medical care for the above named minor child. I authorize the following individual, who is a person over 18. Parent/legal guardian fills out and signs this consent form authorizing up.
Medical Authorization Form For Children Images Medical Free
I have the legal right to consent for medical treatment for this child (patient). Check here if you wish to give consent for the minor to receive medical care without an accompanying adult. _____________________________ (name of caregiver) the right to give consent to authorize medical care for the above named minor child. I authorize the following individual, who is a.
Free Medical Consent for the Treatment of a Minor PDF
I authorize the following individual, who is a person over 18. I have the legal right to consent for medical treatment for this child (patient). Parent/legal guardian fills out and signs this consent form authorizing up health system medical group clinics to provide treatment to. Check here if you wish to give consent for the minor to receive medical care.
Physical Therapy Consent Form Template
_____________________________ (name of caregiver) the right to give consent to authorize medical care for the above named minor child. I have the legal right to consent for medical treatment for this child (patient). Check here if you wish to give consent for the minor to receive medical care without an accompanying adult. Parent/legal guardian fills out and signs this consent.

Consent To Treat A Minor Without Parent Form Ohio 2022 Printable
I authorize the following individual, who is a person over 18. I have the legal right to consent for medical treatment for this child (patient). Parent/legal guardian fills out and signs this consent form authorizing up health system medical group clinics to provide treatment to. Check here if you wish to give consent for the minor to receive medical care.
Printable Medical Consent Form For Minor Printable Forms Free Online
I have the legal right to consent for medical treatment for this child (patient). Parent/legal guardian fills out and signs this consent form authorizing up health system medical group clinics to provide treatment to. Check here if you wish to give consent for the minor to receive medical care without an accompanying adult. I authorize the following individual, who is.
I Authorize The Following Individual, Who Is A Person Over 18.
I have the legal right to consent for medical treatment for this child (patient). Check here if you wish to give consent for the minor to receive medical care without an accompanying adult. Parent/legal guardian fills out and signs this consent form authorizing up health system medical group clinics to provide treatment to. _____________________________ (name of caregiver) the right to give consent to authorize medical care for the above named minor child.